Alzheimers Nursing Care Plan 4y512p
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 3b7i
Overview 3e4r5l
& View Alzheimers Nursing Care Plan as PDF for free.
More details w3441
- Words: 1,376
- Pages: 6
Diagnosis 1. Thought Processes, Altered, related to progressive dementia as evidenced by disorientation to time and place, loss of short-term memory, inability to concentrate, and periods of agitation. DS= her daughter reported that her mother disappeared; Mrs. Rodriguez was agitated and disoriented DO=loss of shortterm memory, inability to concentrate
Goal 1. Mrs. Rodriguez will remain calm and will not experience agitation and anxiety as a result of her disorientation and memory loss.
Intervention 1.1 Provide Mrs. Rodrigues with clues for orientation: “Good morning Mrs. Rodrigues. My name is Devi, and I will help you today.” Avoid putting her on the spot by asking questions she may not answer, such as “Do you know what day this is?” 1.2 Place a large sign on Mrs. Rodriguez’s door with her name printed in large letter to help her find the room.
1.3 Have family bring in snapshots and photos to stimulate reminiscence.
Rationale 1.1 People in the early stages of Alzheimer’s disease may become agitated because their world is always unfamiliar to them. The issue is not whether individuals with a dementia are oriented, but whether they can cope with their environment. 1.2 Short-term memory loss makes it impossible for Mrs. Rodriguez to where her room is or where the bathroom is. If she still recognizes her name, posting it on the door will help her find her way. 1.3 Reminiscing can be a satisfying activity. It is especially helpful if the photos are from an earlier, happier time such as when her children were young. Long-term
Implementation 1.1 Helped the client with ADLs at 7:00 am. - Kristina Devinta, SN (Student Nurse)
1.2 Posted a large print on the client’s door of her name at 7:00 am -Kristina Devinta,SN
1.3 Put up a pictures given by daughter near her bed at 7:30 am -Kristina Devinta, SN
Evaluation 1. S: “my mother becomes calmer.” O: the client does not experience agitation and anxiety’ A: goal met P: continue interventions Mrs. Rodriguez remained calm and showed no signs of agitation or anxiety.
1.4 Avoid changing Mrs. Rodriguez’s room. Put items back in the same place all the time. 1.5 Consult with activities staff in planning selfexpensive, non-fail activities that require little concentration (e.g., painting with non-toxic paints, modeling with nontoxic clay). 1.6 If Mrs. Rodriguez is resistant to care, provide clear, simple, nonthreatening instructions and delay care as needed until she is calmer.
memory may still be intact, allowing her to recall these happier times. 1.4 Consistency in the environment (as well as in routine and staff) reduces frustration. 1.5 Appropriate activities prevent boredom, which can lead to irritation. It is important to plan non-stressful, noncompetitive, failureproof activities in order to prevent frustration. 1.6 Persons with cognitive deficits often vary between combativeness and cooperation. Often, delaying care for even 10 to 15 minutes when resistance is encountered improves client outcomes.
1.4 Cleaned room 305 and prepared it for Mrs Rodriguez at 9:00 am -Kristina Devinta, SN 1.5 Sign up the client for the seminar on May 6, 2011 -Kristina Devinta, SN
1.6 Successfully taught and aided her through the seminar at 4:00 pm -Kristina Devinta, SN
2. Injury, risk for, related to risk factors of mode of transportation and cognitive and affective factors as evidenced by wandering behavior, impaired judgment, and disorientation DS – “Where am I? Why am I here?” DO – client has risk for injury due to wandering off
2. Mrs. Rodriguez will remain free injury while retaining as much independence and freedom as possible.
3. Self-care deficit related to perceptual or cognitive impairment (memory loss and sensoryperceptual deficits) as evidenced by needing a reminder to shower and change clothes. DS – client looks anxious DO – client unable to complete ADL
3. Mrs. Rodriguez will complete ADL with minimal assistance now and with increasing assistance as the disease progresses.
2.1 Look up tools, medicines, and chemicals. Keep only nonpoisonous plants of the unit. Arrange furniture so that walkways are open. Pad sharp corners of Tables and chests. Cover electrical outlets and radiators. Place electrical cords and telephone wires out of reach. 2.2 Provide assurance during free drills.
2.1 Persons with Alzheimer’s disease do not recognize unsafe acts or conditions due to loss of judgment. They do not comprehend cause and effect.
2.1 Prepared room for client at 6:00 am -Samuel Rumahorbo, Student Nurse
2.2 Unusual activity of any sort increases agitation, especially when noise level is increased.
2.2 Help client during free drill at 8:00 am. Samuel Rumahorbo, SN
3.1 Use verbal clues and hand-over-hand assistance with ADL. Instruct staff to avoid doing tasks that Mrs. Rodriguez can do by herself. Watch for signs of frustration and irritation and intervene when appropriate. 3.2 Ask family to bring in clothing that is easy to manipulate.
3.1 Using these simple techniques can minimize the need for assistance, thereby increasing feelings of selfesteem.
3.1 Help client with breakfast and morning walk at 8:15am Samuel Rumahorbo, SN
3.2 Dressing is one of the more difficult tasks to accomplish.
3.2 Aided client in changing clothes at 9:00 am
2. S – “Thank you for helping me, nurse” client is delighted in the nursing home. O – Mrs. Rodriguez has experienced no injury A – Goal met; P – Continue intervention.
3. S - Mrs. Rodriguez participates in ADL with no anxiety O – ADLs are completed A - Goal met; P - Continue intervention
4. Sleep Pattern Disturbance related to disorientation as evidenced by wakefulness at night. DS – client is grouchy in the morning, wakes at night and anxious DO – Client have heavy eye bags and looks drowsy in the morning
4. Mrs. Rodriguez will experience fever periods of wakefulness during the night if she awakens, she will remain calm and free of agitation.
Set clothing out in order it is to be put on. 3.3 Consider tub baths rather than showers. Put privacy and do not leave the client alone.
Appropriate clothing can simplify the activity. 3.3 Showers are frequently threatening or confusing to person with Alzheimer’s disease. Tub baths are also more relaxing.
Samuel Rumahorbo, SN
4.1 Avoid stimulating activities prior to bedtime. Establish a consistent bedtime routine. Take Mrs. Rodriguez to the bathroom and allow sufficient time for complete bladder emptying.
4.1 Overstimulation prior to bedtime may increase anxiety, preventing sleep. Having the client participate in relaxation activities and repeating the client’s long-practiced bedtime routine prior to bed may also be helpful. These activities are relaxing. 4.2Hunger or overeating can interfere with sleep.
4.1 Prepared for bedtime at 8:45pm, brought the client to the bathroom at 8:50pm. -E J Solaiman, SN
4.2 Help Mrs. Rodriguez with a sponge bath and with oral care; give her a back rub using warm lotion and slow, smooth strokes.
3.3 Client took a bath at 8:50 am safely without accident -Samuel Rumahorbo, SN
4.2 Aided the client for a sponge bath, provided oral care, back rub with lotion at 8:55pm -Kristina Devinta, SN
4. S- “I had a wonderful sleep…” O - Mrs. Rodriguez sleeps through the night several times a week; A- Goal met; P - Continue intervention.
4.3 Provide a light snack of a warm, noncaffeinated beverage and a plain, easily digested cracker, cookie, or a piece of toast. Be patient and do not rush her. 4.4 Question family concerning previous bed-time routines and sleeping habits. Repeat bedtime routine when Mrs. Rodriguez awakens during night. 4.5 Encourage a short nap early in the afternoon. 4.6 Avoid the use of sleeping medications.
4.3 Individuals may have used specific sleep routines throughout their lifetimes, such as sleeping with a night light, having a window open, playing a radio, or wearing socks to bed. 4.4 Mrs. Rodriguez will think it is time to go to the bed
4.3 Gave client a whole wheat cracker and a warm glass of water at 9:15pm. -E J Solaiman, SN
4.5 Sleep pattern disturbances may result from over fatigue. 4.6 Sleeping medications are seldom effective and may increase confusion, disorientation, and restlessness.
4.5 Client took a nap at 2:00pm -Samuel Rumahorbo, SN 4.6 Client fell asleep at 9:35pm without the use of medications. -E J Solaman, SN
4.4 Brought client to the bed and prepare for sleep at 9:25pm. -E J Solaiman, SN
Goal 1. Mrs. Rodriguez will remain calm and will not experience agitation and anxiety as a result of her disorientation and memory loss.
Intervention 1.1 Provide Mrs. Rodrigues with clues for orientation: “Good morning Mrs. Rodrigues. My name is Devi, and I will help you today.” Avoid putting her on the spot by asking questions she may not answer, such as “Do you know what day this is?” 1.2 Place a large sign on Mrs. Rodriguez’s door with her name printed in large letter to help her find the room.
1.3 Have family bring in snapshots and photos to stimulate reminiscence.
Rationale 1.1 People in the early stages of Alzheimer’s disease may become agitated because their world is always unfamiliar to them. The issue is not whether individuals with a dementia are oriented, but whether they can cope with their environment. 1.2 Short-term memory loss makes it impossible for Mrs. Rodriguez to where her room is or where the bathroom is. If she still recognizes her name, posting it on the door will help her find her way. 1.3 Reminiscing can be a satisfying activity. It is especially helpful if the photos are from an earlier, happier time such as when her children were young. Long-term
Implementation 1.1 Helped the client with ADLs at 7:00 am. - Kristina Devinta, SN (Student Nurse)
1.2 Posted a large print on the client’s door of her name at 7:00 am -Kristina Devinta,SN
1.3 Put up a pictures given by daughter near her bed at 7:30 am -Kristina Devinta, SN
Evaluation 1. S: “my mother becomes calmer.” O: the client does not experience agitation and anxiety’ A: goal met P: continue interventions Mrs. Rodriguez remained calm and showed no signs of agitation or anxiety.
1.4 Avoid changing Mrs. Rodriguez’s room. Put items back in the same place all the time. 1.5 Consult with activities staff in planning selfexpensive, non-fail activities that require little concentration (e.g., painting with non-toxic paints, modeling with nontoxic clay). 1.6 If Mrs. Rodriguez is resistant to care, provide clear, simple, nonthreatening instructions and delay care as needed until she is calmer.
memory may still be intact, allowing her to recall these happier times. 1.4 Consistency in the environment (as well as in routine and staff) reduces frustration. 1.5 Appropriate activities prevent boredom, which can lead to irritation. It is important to plan non-stressful, noncompetitive, failureproof activities in order to prevent frustration. 1.6 Persons with cognitive deficits often vary between combativeness and cooperation. Often, delaying care for even 10 to 15 minutes when resistance is encountered improves client outcomes.
1.4 Cleaned room 305 and prepared it for Mrs Rodriguez at 9:00 am -Kristina Devinta, SN 1.5 Sign up the client for the seminar on May 6, 2011 -Kristina Devinta, SN
1.6 Successfully taught and aided her through the seminar at 4:00 pm -Kristina Devinta, SN
2. Injury, risk for, related to risk factors of mode of transportation and cognitive and affective factors as evidenced by wandering behavior, impaired judgment, and disorientation DS – “Where am I? Why am I here?” DO – client has risk for injury due to wandering off
2. Mrs. Rodriguez will remain free injury while retaining as much independence and freedom as possible.
3. Self-care deficit related to perceptual or cognitive impairment (memory loss and sensoryperceptual deficits) as evidenced by needing a reminder to shower and change clothes. DS – client looks anxious DO – client unable to complete ADL
3. Mrs. Rodriguez will complete ADL with minimal assistance now and with increasing assistance as the disease progresses.
2.1 Look up tools, medicines, and chemicals. Keep only nonpoisonous plants of the unit. Arrange furniture so that walkways are open. Pad sharp corners of Tables and chests. Cover electrical outlets and radiators. Place electrical cords and telephone wires out of reach. 2.2 Provide assurance during free drills.
2.1 Persons with Alzheimer’s disease do not recognize unsafe acts or conditions due to loss of judgment. They do not comprehend cause and effect.
2.1 Prepared room for client at 6:00 am -Samuel Rumahorbo, Student Nurse
2.2 Unusual activity of any sort increases agitation, especially when noise level is increased.
2.2 Help client during free drill at 8:00 am. Samuel Rumahorbo, SN
3.1 Use verbal clues and hand-over-hand assistance with ADL. Instruct staff to avoid doing tasks that Mrs. Rodriguez can do by herself. Watch for signs of frustration and irritation and intervene when appropriate. 3.2 Ask family to bring in clothing that is easy to manipulate.
3.1 Using these simple techniques can minimize the need for assistance, thereby increasing feelings of selfesteem.
3.1 Help client with breakfast and morning walk at 8:15am Samuel Rumahorbo, SN
3.2 Dressing is one of the more difficult tasks to accomplish.
3.2 Aided client in changing clothes at 9:00 am
2. S – “Thank you for helping me, nurse” client is delighted in the nursing home. O – Mrs. Rodriguez has experienced no injury A – Goal met; P – Continue intervention.
3. S - Mrs. Rodriguez participates in ADL with no anxiety O – ADLs are completed A - Goal met; P - Continue intervention
4. Sleep Pattern Disturbance related to disorientation as evidenced by wakefulness at night. DS – client is grouchy in the morning, wakes at night and anxious DO – Client have heavy eye bags and looks drowsy in the morning
4. Mrs. Rodriguez will experience fever periods of wakefulness during the night if she awakens, she will remain calm and free of agitation.
Set clothing out in order it is to be put on. 3.3 Consider tub baths rather than showers. Put privacy and do not leave the client alone.
Appropriate clothing can simplify the activity. 3.3 Showers are frequently threatening or confusing to person with Alzheimer’s disease. Tub baths are also more relaxing.
Samuel Rumahorbo, SN
4.1 Avoid stimulating activities prior to bedtime. Establish a consistent bedtime routine. Take Mrs. Rodriguez to the bathroom and allow sufficient time for complete bladder emptying.
4.1 Overstimulation prior to bedtime may increase anxiety, preventing sleep. Having the client participate in relaxation activities and repeating the client’s long-practiced bedtime routine prior to bed may also be helpful. These activities are relaxing. 4.2Hunger or overeating can interfere with sleep.
4.1 Prepared for bedtime at 8:45pm, brought the client to the bathroom at 8:50pm. -E J Solaiman, SN
4.2 Help Mrs. Rodriguez with a sponge bath and with oral care; give her a back rub using warm lotion and slow, smooth strokes.
3.3 Client took a bath at 8:50 am safely without accident -Samuel Rumahorbo, SN
4.2 Aided the client for a sponge bath, provided oral care, back rub with lotion at 8:55pm -Kristina Devinta, SN
4. S- “I had a wonderful sleep…” O - Mrs. Rodriguez sleeps through the night several times a week; A- Goal met; P - Continue intervention.
4.3 Provide a light snack of a warm, noncaffeinated beverage and a plain, easily digested cracker, cookie, or a piece of toast. Be patient and do not rush her. 4.4 Question family concerning previous bed-time routines and sleeping habits. Repeat bedtime routine when Mrs. Rodriguez awakens during night. 4.5 Encourage a short nap early in the afternoon. 4.6 Avoid the use of sleeping medications.
4.3 Individuals may have used specific sleep routines throughout their lifetimes, such as sleeping with a night light, having a window open, playing a radio, or wearing socks to bed. 4.4 Mrs. Rodriguez will think it is time to go to the bed
4.3 Gave client a whole wheat cracker and a warm glass of water at 9:15pm. -E J Solaiman, SN
4.5 Sleep pattern disturbances may result from over fatigue. 4.6 Sleeping medications are seldom effective and may increase confusion, disorientation, and restlessness.
4.5 Client took a nap at 2:00pm -Samuel Rumahorbo, SN 4.6 Client fell asleep at 9:35pm without the use of medications. -E J Solaman, SN
4.4 Brought client to the bed and prepare for sleep at 9:25pm. -E J Solaiman, SN
Related Documents 3m3m1z

Alzheimers Nursing Care Plan 4y512p
October 2019 169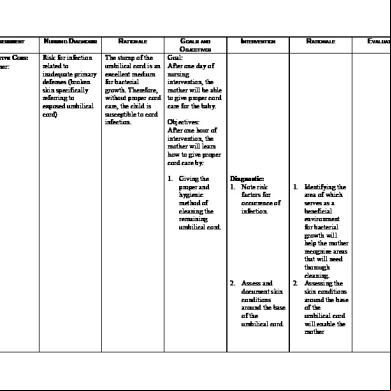
Nursing Care Plan Cord Care 6l3w3i
December 2019 850
Craniotomy Nursing Care Plan t632d
December 2021 0
Nursing Care Plan 636zq
January 2022 0
Nursing Care Plan Fatigue 5n3j73
November 2021 0
Fever Nursing Care Plan 2n4q1x
October 2019 1,488More Documents from "Jethro Solaiman" x1u6p
Alzheimers Nursing Care Plan 4y512p
October 2019 169
Introduction Broken Homes 6d4v1v
December 2019 17
Foreign Chapter 2 601w3q
September 2020 0
Heneral Luna Reaction Paper 3h3924
October 2019 8,888
What Is In Situ Soil Testing 39ei
November 2019 82