Dr Is-acute Pancreatitis 83968
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 3b7i
Overview 3e4r5l
& View Dr Is-acute Pancreatitis as PDF for free.
More details w3441
- Words: 404
- Pages: 11
Acute Pancreatitis dr. Isbandiyah, SpPD FK UMM
CAUSES OF ACUTE NECROTIZING PANCREATITIS.
Most common
• Choledocholithiasis • Ethanol abuse • Idiopathic
Less common • • • •
Post Endoscopic retrograde cholangiopancreatography Hyperlipidemia hypercalcemia Drugs (azathioprine, sulfonamides, thiazide, methildopa, estrogen, NSAID) • Pancreas divisum • Abdominal trauma
Least common
• Hereditary (familial)
Clinical Manifestations
Acute pancreatitis usually has a rapid onset Acute pancreatitis may be clinically mild or severe Manifested by upper abdominal pain, vomiting, fever, tachycardia, leukocytosis, and elevated serum levels of pancreatic enzymes
Diagnose
Clinical manifestations Lab. Finding USG CT-scan
CLASSIFICATION
Classifications for acute pancreatitis are used to identify patients at risk for complications. Ranson’s score is based on 11 clinical signs with prognostic importance; 5 are measured at the time of ission and the other 6 in the first 48 hours after ission Acute Physiology and Chronic Health Evaluation (APACHE II) score
Ranson’s score
Ranson’s score »3 (Ranson’s criteria of severity: at ission) • • • • •
Age >55 yr, white-cell count >16,000/mm3 blood glucose >200 mg/dl (11.1 mmol/liter), serum LDH >350 IU/liter serum AST >250 IU/liter
During initial 48 hr
• absolute decrease in hematocrit >10%, • increase in blood urea nitrogen >5 mg/dl (1.8 mmol/liter), • serum calcium <8 mg/dl (2 mmol/liter), • arterial PaO2 <60 mm Hg, • base deficit >4 mmol/liter, • fluid sequestration >6 liters
APACHE II A. Acute physiology score Temperature-rectal Mean arterial pressure Heart rate Respiratory rate Oxygenation Arterial PH Serum sodium Serum potasium Hematocrit White blood count GCS Serum HCO3
B. Age points < 44 45-54 55-64 64-74 >75
0 2 3 5 6
C. Chronic health points (history of severe organ system insufficiency)
Complication
Systemic complications • Acute respiratory distress syndrome • Acute renal failure, • Shock, • Coagulopathy, • Hyperglycemia, and • hypocalcemia.
Local complications • Gastrointestinal bleeding • Infected necrosis, • Adjacent bowel necrosis. • pancreatic abscess • Pancreatic pseudocysts.
MANAGEMENT
ive care • • • •
Analgesics Antibiotics Fasting Nutritional (parenteral nutrition, or enteral feeding by nasoenteric tube)
Endoscopic retrograde cholangiopancreatography (ER) and biliary sphincterotomy in patients with acute gallstone pancreatitis and choledocholithiasis Débridement of infected necrosis
• Operative management (explorative and drainage) • Alternative techniques of débridement (percutaneous or endoscopic)
CAUSES OF ACUTE NECROTIZING PANCREATITIS.
Most common
• Choledocholithiasis • Ethanol abuse • Idiopathic
Less common • • • •
Post Endoscopic retrograde cholangiopancreatography Hyperlipidemia hypercalcemia Drugs (azathioprine, sulfonamides, thiazide, methildopa, estrogen, NSAID) • Pancreas divisum • Abdominal trauma
Least common
• Hereditary (familial)
Clinical Manifestations
Acute pancreatitis usually has a rapid onset Acute pancreatitis may be clinically mild or severe Manifested by upper abdominal pain, vomiting, fever, tachycardia, leukocytosis, and elevated serum levels of pancreatic enzymes
Diagnose
Clinical manifestations Lab. Finding USG CT-scan
CLASSIFICATION
Classifications for acute pancreatitis are used to identify patients at risk for complications. Ranson’s score is based on 11 clinical signs with prognostic importance; 5 are measured at the time of ission and the other 6 in the first 48 hours after ission Acute Physiology and Chronic Health Evaluation (APACHE II) score
Ranson’s score
Ranson’s score »3 (Ranson’s criteria of severity: at ission) • • • • •
Age >55 yr, white-cell count >16,000/mm3 blood glucose >200 mg/dl (11.1 mmol/liter), serum LDH >350 IU/liter serum AST >250 IU/liter
During initial 48 hr
• absolute decrease in hematocrit >10%, • increase in blood urea nitrogen >5 mg/dl (1.8 mmol/liter), • serum calcium <8 mg/dl (2 mmol/liter), • arterial PaO2 <60 mm Hg, • base deficit >4 mmol/liter, • fluid sequestration >6 liters
APACHE II A. Acute physiology score Temperature-rectal Mean arterial pressure Heart rate Respiratory rate Oxygenation Arterial PH Serum sodium Serum potasium Hematocrit White blood count GCS Serum HCO3
B. Age points < 44 45-54 55-64 64-74 >75
0 2 3 5 6
C. Chronic health points (history of severe organ system insufficiency)
Complication
Systemic complications • Acute respiratory distress syndrome • Acute renal failure, • Shock, • Coagulopathy, • Hyperglycemia, and • hypocalcemia.
Local complications • Gastrointestinal bleeding • Infected necrosis, • Adjacent bowel necrosis. • pancreatic abscess • Pancreatic pseudocysts.
MANAGEMENT
ive care • • • •
Analgesics Antibiotics Fasting Nutritional (parenteral nutrition, or enteral feeding by nasoenteric tube)
Endoscopic retrograde cholangiopancreatography (ER) and biliary sphincterotomy in patients with acute gallstone pancreatitis and choledocholithiasis Débridement of infected necrosis
• Operative management (explorative and drainage) • Alternative techniques of débridement (percutaneous or endoscopic)
Related Documents 3m3m1z
Dr Is-acute Pancreatitis 83968
December 2022 0
Pancreatitis 4s5l5x
October 2019 32
Pancreatitis 4s5l5x
August 2021 0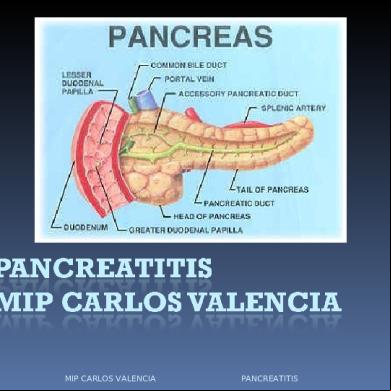
Pancreatitis 4s5l5x
July 2021 0
Pancreatitis 4s5l5x
April 2021 0
Pancreatitis. 6gp3z
July 2021 0More Documents from "Semesta " 46304v
Dr Meddy Leukemia 3z3035
July 2021 0
Dr Is-acute Pancreatitis 83968
December 2022 0